

Background:
Conditioning regimen given before allogeneic hematopoietic stem cell transplantation (allo-HSCT) contributes significantly to the outcomes following transplant for myelodysplastic syndrome (MDS). Myeloablative conditioning (MAC) regimens are often associated with a lower risk of relapse; however, their use is often limited by toxicity and a higher risk of non-relapse mortality (NRM). Reduced-intensity conditioning (RIC) regimens are associated with a higher risk of relapse, a lower NRM, a lower incidence of graft versus host disease (GVHD), and hence is feasible in patients with advanced age or comorbidities. This study highlights the importance of the difference between the two interventions used in allo-HSCT for myelodysplastic syndrome (MDS).
Methods:
We conducted a comprehensive literature search using PubMed, Clinicaltrial.gov, Embase, Cochrane, and Web of Science on 5th May 2020 with no restriction of language or period. Initial research revealed 1698 articles. After excluding review articles, duplicates, and non-relevant articles, we included two randomized clinical trials and three cohort studies, which reported overall survival (OS), relapse-free survival (RFS), relapse incidence (RI), and incidence of acute and chronic (GVHD). Based on inclusion criteria, two randomized clinical trials (BMT CTN 0901 Trial Scott et al. 2017 & EBMT RICMAC Trial Kroger et al. 2017) and three cohort studies (BBMT 55226 Park et al. 2018, BBMT Orozco et al. 2019, BMT Alatrash et al. 2019) were included.
Results:
Among combined MDS and acute myeloid leukemia (AML) patients (n=1188) enrolled in 5 studies, 651 patients had MDS. Patients underwent MAC (n=484) or RIC (n=692) followed by either a matched related donor (MRD), n=236, or matched unrelated donor (MUD), n=236, allo-HCT. The median age range at the time of transplant was 50-54 years
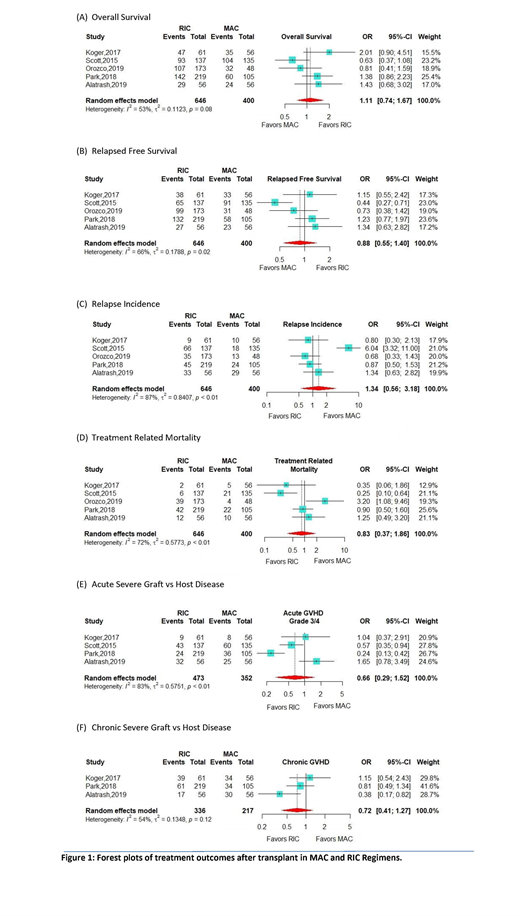
The use of RIC causes statistically non-significant trend of improved overall survival (OS) (OR 1.11: 95% CI: 0.74-1.67, p-value= 0.61) along with more risk of relapse incidence (RI) (R 1.34: 95% CI: 0.56-3.18, p value= 0.51), and reduced relapse free survival (RFS) (OR 0.88, 95% CI: 0.55-1.44: p value= 0.59). Differences were found in terms of safety of both conditioning regimens. MAC allo-HCT have more acute GVHD, grade 3 and 4 (OR 0.66: 95% CI: 0.29-1.52, p value= 0.33) and chronic GVHD, grade 3 and 4 (OR 0.72: 95% CI: 0.41-1.27: p value= 0.26) and treatment-related mortality (TRM) (OR 0.83, 95% CI: 0.37-1.86, p value= 0.65). The meta-analysis results are shown in figure-1.
Conclusion: In adult MDS patients undergoing allo-HSCT, RIC is associated with improved overall survival, but at the cost of reduced RFS, and a higher risk of relapse. MAC, on the other hand, is associated with more treatment-related mortality and GVHD. Results of our analysis point out these trends but these are not statistically significant
Anwer:Incyte, Seattle Genetics, Acetylon Pharmaceuticals, AbbVie Pharma, Astellas Pharma, Celegene, Millennium Pharmaceuticals.: Honoraria, Research Funding, Speakers Bureau.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal